Confirmation
Download PDF
Open All
PR35: Bladder Pressure Monitoring
Applicable To
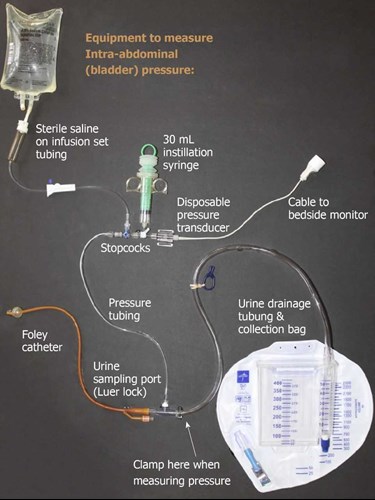
Introduction
Bladder pressure monitoring is used to identify an often under-recognized and under-treated cause of obstructive shock related to intra-abdominal hypertension. Intra-abdominal pressure (IAP) is graded by:
- Grade I: 12-15 mmHg
- Grade II: 16-20 mmHg
- Grade III: 21-25 mmHg
- Grade IV: > 25 mmHg
Abdominal compartment syndrome is a sustained IAP of more than 20 mmHg and is associated with new organ dysfunction. Consideration needs to be paid to a primary or secondary cause so that appropriate treatment can be initiated. Reducing the obstructive shock state allows for a safer conveyance.
Indications
- Suspected obstructive shock resulting from either a primary or secondary source of abdominal hypertension that has led to abdominal compartment syndrome
Contraindications
- Any patient unable to tolerate a head-of-bed < 20°
Caution: a blocked or kinked Foley will give falsely high pressures
Caution: PEEP will cause falsely high pressures
Procedure
- Perform hand hygiene.
- Patient should be placed in the supine position for measurement. The head of the bed needs to be < 20°. If this is not clinically feasible, it is important to recognize that elevation of the head of the bed will result in a higher IAP.
- Document position and ensure all subsequent readings are taken in the same position.
- Prime the pressure monitoring tubing.
- Connect the tubing to the sampling port on the Foley tubing using aseptic technique.
- Connect the transducer cable to the monitor.
- Level at the cross section of the mid-axillary line and the iliac crest; zero the transducer.
- Change the scale on the monitor to 30 mmHg.
- Clamp the drainage tube to the urine bag below or distal to the sampling port.
- Using the port on the tubing and the three-way stopcock, fill the bladder with 1mL/kg (minimum of 3 mL and maximum 25 ml) of 0.9% sterile sodium chloride using the syringe. The volume of fluid in the bladder should be constant for each subsequent measurement.
- Once instilled, close the stopcock of the syringe and wait 60 seconds.
- Obtain the mean pressure reading upon end expiration.
- The abdominal pressure should produce fluctuations in the waveform.
- Once finished with the reading, re-open the clamp.
Notes
- False positives can occur with patient position, RASS, and detrusor muscle contraction.
- Some commercial products connect directly in line with the Foley tubing.
Resources
References
- Gestring M. Abdominal compartment syndrome in adults. 2020. [Link]
- Raccanello J., Morris K. Intra-abdominal pressure monitoring. 2020. [Link]
- Morgan B. Information and procedure: intra-abdominal pressure monitoring. [Link]
- Rogers WK, Garcia L. Intraabdominal hypertension, abdominal compartment syndrome, and the open abdomen. 2018. [Link]