Confirmation
Download PDF
Open All
PR42: EVD Monitoring and Drainage
Applicable To
Introduction
An external ventricular drain (EVD) is a small catheter inserted through the skull, usually into the lateral ventricle, which is typically connected to a collecting device to allow for drainage of cerebrospinal fluid. The EVD can also be connected to a transducer that monitors and records ICP. This allows ICP monitoring and guidance of ICP management using the equation CPP = MAP – ICP. Cerebral perfusion can thus be guided with osmotherapy, hypertonic solutions, and vasopressors to avoid herniation and cerebral ischemia. CSF can also be drained to avoid further herniation. The overall management allows for parenchymal fluid shift, CSF drainage, and hemodynamic optimization to improve cerebral blood flow.
Indications
- Currently limited locations can insert or monitor such devices; as such it must be in situ prior to the transfer
- Hydrocephalus and neurologic decline
- TBI with a GCS ≤ 8 and an abnormal CT scan showing evidence of mass effect
- Following surgery, particularly tumor surgery, until the CSF circulation is re-established
- To enable drainage of infected CSF
- In patients with a severe head injury to provide both a means of measuring ICP and allowing CSF drainage to treat raised ICP
- ICP monitoring in severe TBI patients with a normal CT scan may be indicated if two of the following features are present: age > 40 years; motor posturing; systolic blood pressure < 90 mmHg
Contraindications
- A patient receiving anticoagulation therapy
- A scalp infection
- Caution: Caution must be used with continuous drainage since excessive drainage can lead to ventricular collapse and malfunctioning, or occlusion, of the catheter in the setting of cerebral edema in small ventricles. In the conveyance environment, the patient will not be level at all times. Therefore, continuous drainage should be avoided.
Procedure
Consult with appropriate neurological service for specific instructions and care planning during conveyance.
1. Errors in positioning the transducer:
- Too far above the foramen of Monro (FOM) will lead to a falsely low ICP measurement and insufficient drainage of CSF. In this case, intracranial hypertension would go undetected and untreated.
- Too far below the FOM will lead to a falsely high ICP measurement and excessive drainage of CSF. This may collapse the ventricles and possibly induce blockage of the system resulting in unnecessary treatments.
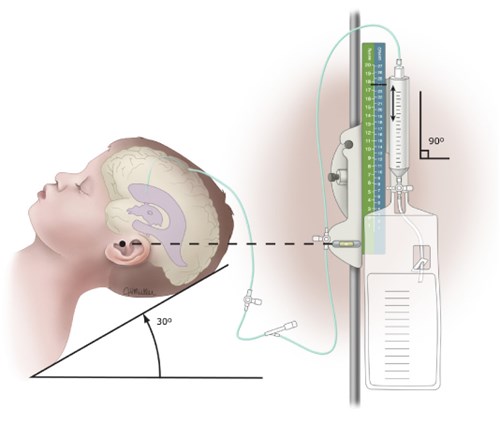
2. Leveling procedure:
- Explain to the patient/family what is about to occur.
- Perform hand hygiene.
- Turn on the laser (protect the patient’s eyes from the laser).
- Ensure the level is horizontal and the bubble is centred between the lines.
- Turn the 3-way stopcock between the patient and the burette on the EVD system to the off position, preventing the flow of CSF.
- Alter the height of the entire EVD system to bring the transducer laser horizontal with the patient’s FOM. (Supine = tragus of the ear; lateral = midsagittal line, between the eyebrows.)
- Once levelled, turn the 3-way stopcock between the patient and the burette on the EVD system to the on position, allowing the flow of CSF.
- This procedure needs to be followed at the beginning of the transfer and every time the patient moves or is moved.
3. Monitoring:
- Set the burette level appropriate for the individual needs. Often 15-20, but this will be patient dependent. Note the monitoring units of the burette, either cmH2O or mmHg. The difference is 1.36. The monitor will measure in mmHg and if the burette is in cmH2O, an ongoing calculation will have to be made to ensure accidental drainage does not occur.
- Once leveled, zero the transducer.
- Ensure connections are secure.
- Turn monitor on and ensure appropriate ICP cords are connected.
- Set appropriate alarm limits (including ICP limits).
- Perform hand hygiene.
- Zero on the monitor:
- Turn stopcock off.
- Lower the drip chamber until the pressure indicator window is centred over the 0 position on the pressure scale.
- Press zero on the monitor.
- Once the pressure transducer is zeroed, the drip chamber needs to be raised back to the desired setting.
- Turn the EVD stopcock to the off position. This will allow a pressure to be read on the monitor.
- The off position should be utilized for conveyance as bumps in the road, takeoffs, and landings will alter patient positioning and thus leveling. The off position will ensure that inadvertent drainage will not occur.
- If the ICP is increasing and drainage is required, first ensure the patient and transducer are leveled.
- If opening the stopcock for CSF drainage due to increasing ICP, turn the EVD on and ensure the drain is oscillating/draining. Keep in mind CSF is produced at a rate of 20 mL/hour.
- Key point: ICP cannot be measured if the EVD is open or on continuous drainage.
- Once opened and the goal of care is met, reset the stopcock to the closed position.
Notes
- The major complications associated with EVD use are catheter occlusion, due to clotted blood at the intraventricular orifice, and infection.
- Be aware of excessive CSF drainage if the drain is left open or inappropriately leveled.
- Patients with more severely impaired autoregulation and suboptimal CPP are best managed with efforts to lower ICP, rather than by elevating MAP with vasopressors; hypertension is more likely to worsen cerebral edema when protective autoregulation is impaired.
- An ICP goal ≤ 22 mmHg is recommended as the threshold that predicts survival and a favourable outcome following TBI. Individual goals need to be discussed with ETP.