Confirmation
CBRNE Emergencies
Reviewed: October 2025
Introduction
This CPG is designed to guide BCEHS paramedics in recognizing, triaging, and treating casualties during Chemical, Biological, Radiological, Nuclear, and Explosive (CBRNE) incidents, while ensuring responder safety and coordination with partner agencies.
A CBRNE incident involves the deliberate release of hazardous agents: chemical, biological, radiological, nuclear, or explosive. And typically with malicious intent, such as terrorism. This differs from a HazMat event, which generally results from accidental release during industrial or transportation incidents. Each CBRNE agent type poses unique risks: chemical agents cause rapid toxicity, biological agents spread disease, radiological and nuclear materials lead to radiation exposure, and explosives cause traumatic injuries and contamination.
For paramedics, the priorities are early hazard recognition, strict scene discipline, and life-saving care while preventing further harm or contamination. These events also pose significant operational challenges for BCEHS, including responder safety, system capacity, and public confidence. Large-scale incidents require sustained coordination with police, fire, emergency management, and health authorities.
Guiding Principles
- Safety First: Medical care by BCEHS Paramedics occurs only in the Cold Zone. Early consultation with CliniCall/Paramedic Specialist is high recommended; ideally en-route to the scene. Staging of vehicles should be up-wind, up-hill or up-stream.
- Phased Care: Focus on Direct Threat → Indirect Threat → Evacuation phases rather than rigid zones.
- Life Before Limb: Prioritize airway, hemorrhage control, and stabilization over complete decontamination.
- Scalable Response: Adjust interventions to available PPE, training, and local conditions.
- Antidote Therapy: If available and within scope, consider MCM use
- Documentation: Clearly record agent type (if known), decontamination method, and treatment timeline.
Under no circumstances are BCEHS Paramedics authorized to practice in the HOT Zone
This CPG aligns with the Tactical Emergency Casualty Care (TECC) framework and complements the BCEHS Mass Casualty Incident and Active Direct Threat info.
Scene Safety & Risk Awareness
Do NOT enter a contaminated environment without appropriate training and PPE.
CBRNE recognition includes observing for unusual odours, mists, vapour clouds, clustering of patients with similar symptoms, and environmental indicators (dead animals, vegetation die-off, etc.).
Zoning: Identify safe distances for crew safety. Identify & confirm location of Hot, Warm & Cold Zones with partner agencies. Warm zone interventions may occur before or during decontamination (DECON) based on risk assessment and tactical feasibility.
- Hot Zone
- Area of highest contamination or exposure which is Immediately Dangerous to Life or Health (IDLH); only personnel in full PPE may enter to perform lifesaving actions and rapid evacuation.
Example: Inside a laboratory where a biological agent such as anthrax has been released into the air.
- Area of highest contamination or exposure which is Immediately Dangerous to Life or Health (IDLH); only personnel in full PPE may enter to perform lifesaving actions and rapid evacuation.
- Warm Zone
- Transition area where decontamination and limited medical care occur using appropriate PPE before patients move to the clean area.
Example: Decontamination corridor set up outside the building where responders assist potentially exposed individuals before entry to the safe zone.
- Transition area where decontamination and limited medical care occur using appropriate PPE before patients move to the clean area.
- Cold Zone
- Safe area free of contamination where full assessment, treatment, and patient transport take place.
Example: Medical treatment area established beyond the decontamination line where patients are clinically managed and prepared for hospital transport.
- Safe area free of contamination where full assessment, treatment, and patient transport take place.
Operational Priorities
Safety of responders always takes precedence.
Triage and rapid evacuation of viable patients improves outcomes.
Coordinate with HazMat / DECON teams for patient flow and contamination control.
Documentation should clearly note suspected agents, decontamination status, and treatment timelines.
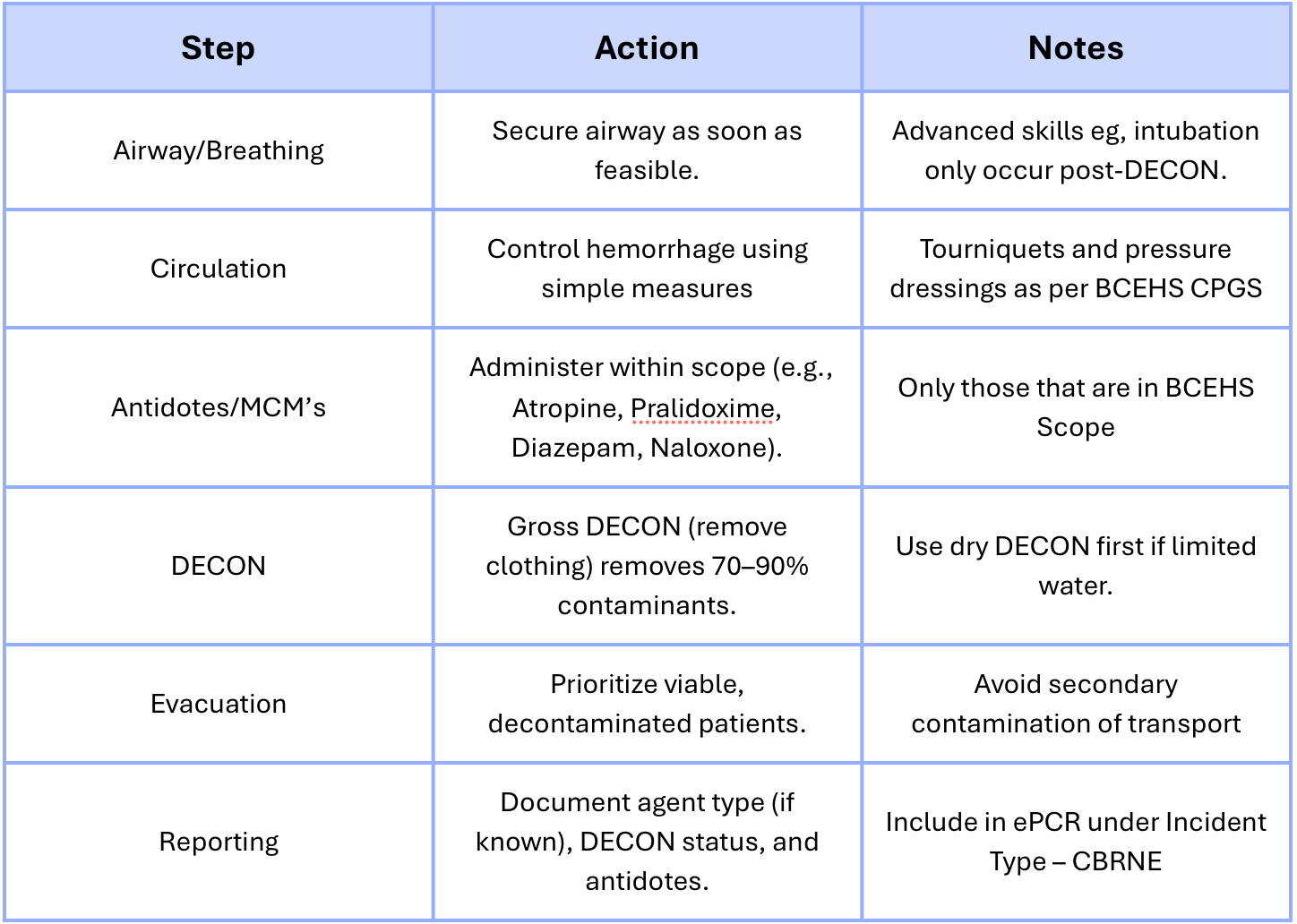
Medical Management
Early airway and breathing support remain critical; contamination should not delay life-saving interventions if safe to perform. Don’t delay treatment, don’t delay transport. See B01: Airway Management for interventions
Medical Counter-Measure (MCM) administration (e.g., atropine, pralidoxime, benzodiazepines, naloxone) should occur per BCEHS scope and available stock. See CPGs J:Poisonings & Toxic Exposures for further into.
DECON Procedure
Crew MUST contact CliniCall prior to commencing decontamination activities.
Gross decontamination (removal of outer clothing) eliminates 70–90% of contaminants.
Dry decontamination may precede wet DECON if water resources are limited.
Secondary triage occurs post-DECON to identify latent or delayed presentations.
Remote medical assessment may be required where patient access is delayed due to contamination risk.
Special Note: consider the risk/effects of off-gasing based on transport vehicle i.e. confined space, aircraft (i.e. pilots).
Specific Considerations:
Chemical Agents: Nerve, blister, choking, blood, and incapacitating agents.
Biological Agents: Pathogens transmitted via inhalation or contact; consider delayed onset.
Radiological/Nuclear: Prioritize life-threat interventions over contamination; external exposure vs. internal contamination require different management.
Pharmaceutical-Based Agents (PBAs): Includes synthetic opioids; naloxone availability and crew protection are essential.
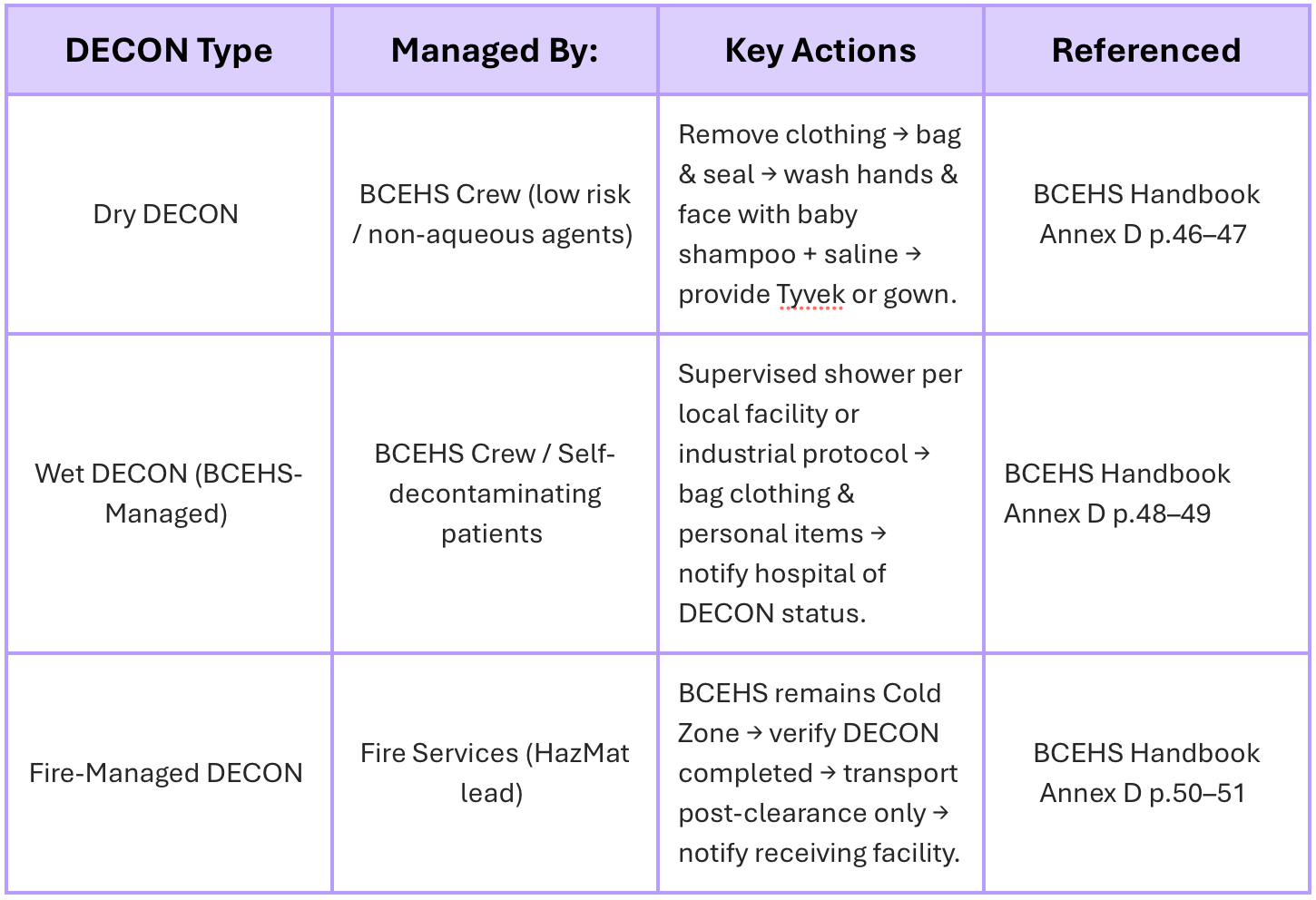
Decontamination (DECON) Procedures
Procedures align with BCEHS Handbook Annex D (2016), including dry and wet DECON steps based on risk assessment. Refer to Annex D for full operational instructions.
CBRNE Incident Flow:
- Recognize → Unusual signs, symptoms, or clustering
- Protect → PPE, zoning, and safety first
- Decontaminate → Remove clothing, rinse or blot as appropriate
- Triage → Prioritize based on viability and contamination level
- Treat → Airway, antidotes, bleeding control
- Transport → Clean corridor → receiving facility
- Report → Patient exposure details and DECON status